 Italiano
Italiano
 English
English
 Français
Français
 Русский
Русский
 Română
Română





Article published in the medical assistance
F Braccini, R Braccini, Saban Y.
What to do before a dysphonia.
Concours Médical 2001; 34, 2288-93.
* Frédéric Braccini, Rosine Braccini **, Yves SABAN *.
* ENT – Neck Surgery
4 avenue Georges Clemenceau – 06000 NICE
** SPEECH
The Regina 71 Boulevard de Cimiez – 06000 NICE
Dysphonia is a temporary or permanent impairment of vocal function experienced by the subject or his entourage. This disorder involves one or more acoustic characteristics of voice (pitch, timbre and intensity).
This is the earliest clinical sign in cancers of the larynx. However, despite its alarming nature, dysphonia is often the expression of a pathology quite benign.
To assert the origin of the laryngeal dysphonia, should be eliminated:
a flow problem related to pulmonary respiratory failure
rhinolalia an open (articulation disorder of speech due to insufficient velar)
rhinolalia a closed (obstacle in the cavum)
I-Duties of the Larynx
The larynx is involved in four essential functions: breathing, swallowing, phonation andeffort closure.
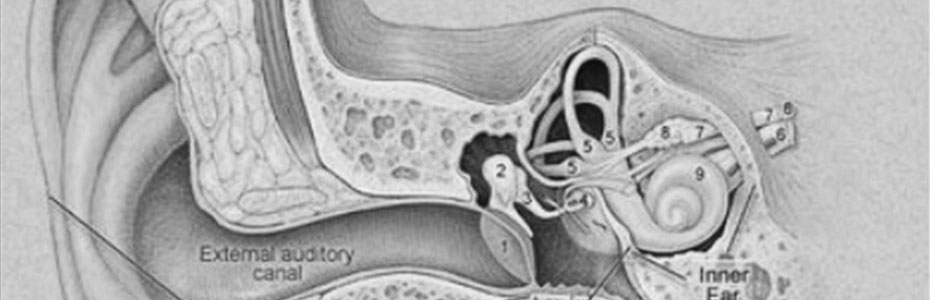
II-Anatomy
a. The Larynx
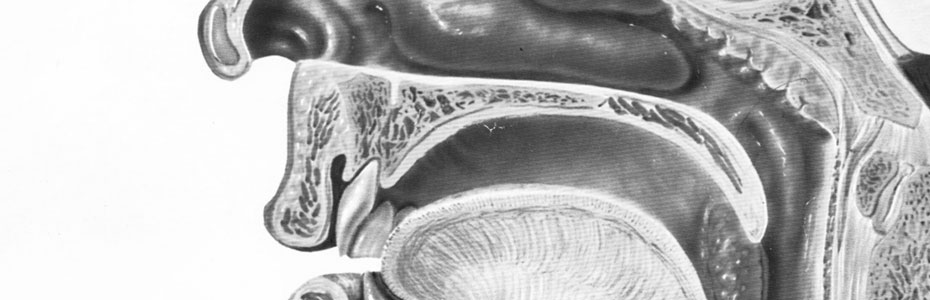
The larynx is a fragment of a cylinder placed in the wake of the trachea in the neck, andopens above the resonant cavities (pharynx, mouth and secondarily, nasal)
The vocal cords divide the laryngeal cavity in three stages:
– an upper floor or laryngeal vestibule
– a mid-level or stage glottic
– a lower level or sub-glottis
The vestibule is formed by the epiglottis forward aryteno-epiglottic folds laterally and the inter-arytenoid notch back.
The glottis is between the free edges of the vocal cords and forth between the voice ofapophyses arytenoids.
Sub-glottis meets up to the vocal cords, down to the cricothyroid membrane and the inner surface of the cricoid cartilage.
b.La laryngeal musculature
The muscles are functionally separated into 3 parts as they are:
Tensors of the vocal cords: the cricothyroid muscle
Constrictors of the glottis: crico-arytenoid lateral thyro-arytenoid muscles inferior, superior thyro-arytenoid muscles, muscle aryepiglottic
Dilator of the glottis: the posterior cricoarytenoid muscle
c.La laryngeal mucosa
The mucosa consists of a respiratory epithelium, ciliated except at the free edge of the vocal cords and the laryngeal surface of the epiglottis where it is stratified squamous.
d.La Vascularization
Vascularization supraglottic is achieved by superior laryngeal artery from the superior thyroid and external carotid.
Vascularization is subglottic laryngeal artery by less than from the inferior thyroid artery and the subclavian artery.
e. The innervation
It comes from the vagus nerve (X).
The superior laryngeal nerve has a sensory branch to branch and endolarynx external drive not participating in the mobility of the vocal cords.
The inferior laryngeal nerve or recurrent laryngeal nerve is actually the most important, it provides the motor innervation of the vocal cords. Its path is not symmetrical: on the right it forms a loop under the subclavian artery and left, it goes down lower in the chest and back (“recurrent”) passing under the arch of the aorta.
III-Diagnosis of Dysphonia
a.Interrogatoire
He stated age, looking for factors promoting dysphonia (chronic factors):
Malmenage-voice “voice miss use” (bad vocal technique)
Voice-overwork “voice abuse” (socio-professional obligation to speak)
-Difficult acoustic conditions (work on projects in the noise, teachers in lecture halls …)
-Exposure to dust and pollutants
Smoking-intoxication
Chronic-sphere O.R.L
-Gastroesophageal reflux disease (GERD)
Loop-audio-phonatory defective (hearing loss embarrassing topic of assessment of the parameters of his voice, the intensity is often causing increased forcing voice)
Mode-family communication (shouting …)
This examination should also identify factors that can trigger sudden dysphonia, events more or less spot on the occasion of which can be a vicious cycle of forcing voice:
– Voice-acute trauma (excessive voice, intubation)
– Psychological factors (“the emotion is happy in the throat”)
– Acute laryngitis tracheitis
b.Examen clinical
The subjective analysis of dysphonia (spoken voice, singing voice) will focus on the following criteria:
-Height: loss of acute and / or voice very aggravated (nodules, Reincke’s edema), or modulated monotone …
-Stamp: veiled (glottal leakage), blown (open bite), frayed, Nason (velar insufficiency), quavering (neurological) ….
-Intensity: Low (hypophonic), or conversely high (children criers …), damage of any “final”.
It will be appreciated the type of patient breathing (upper thoracic, costo-diaphragmatic) and posture (position of the chin, shoulders, trunk).
The inspection involved a random search, a turgor of the jugular veins or muscle tension in the neck forcing witnesses a voice.
Palpation search lymphadenopathy or brain tumor (thyroid) …
The existence of a cough when fluid intake is suggestive of a vocal cord paralysis.
Laryngeal examination is essential and is carried out:
or by indirect laryngoscopy with a mirror, made in consultation with laryngeal mirrors.The laryngeal mirror, previously heated (to prevent fogging) is applied against the posterior wall of the oropharynx, by repressing the uvula. The observation of the larynx in phonation (vocal fold closing) is done by asking the patient to pronounce a / e / or / i / view and examination of the larynx in respiration (vocal cords open) requires a mouth breathing without noise.
This routine is not feasible in children under 6 years in the subject or nauseous when there are anatomical variants (limited mouth opening, macroglossia, epiglottis tilted back …)
Or by indirect laryngoscopy rigid tube (épipharyngoscope)
The endoscope is inserted into the mouth under the arches of a sail in paramedian position. We can see the entire pharyngo-larynx with great accuracy. The magnification can detect anomalies chordal invisible mirror. The limitations of this review are identical to those of the mirror.
Or through the flexible tube nasofibroscopie
Probe 3 mm in diameter is inserted into a nostril of the patient. This approach has the advantage of less well defined to allow the observation of the larynx during phonation and singing.
These two tests are complementary and in most cases an accurate inspection of the larynx without any special preparation. One can, in some people highly reactive, help a local anesthetic to reduce contact the gag reflex.
The laryngostroboscopie
During phonation, the chordal vibration of the mucosa is greater than 100 cycles / second, which is unobservable to the naked eye. The strobe light allows the study of this movement by breaking down the movement in slow motion or by freezing. Thus, one can see the irregularities of the mucosa, the ripple, the symmetry of movement and vibration amplitude of the vibration.
Direct laryngoscopy under general anesthesia

The laryngoscope is inserted into the mouth and pharynx in raising the epiglottis. Using the operating microscope binocular provides perfect vision of the lesions, an accurate assessment of extensions of cancer and the biopsy (essential) and allows acts of laryngeal microsurgery (instrumental or laser).
c. additional examens
Exploration electric larynx
It is mainly used in laryngeal pathology of neurological (MS, Parkinson’s disease …)
The electroglottography: two electrodes are placed on the neck of both sides of the thyroid cartilage, then sends a high frequency current.
Laryngeal Electromyography: collects directly the action potentials of the laryngeal muscles by inserting needles from them. This is useful in the peripheral or centralneurological motor skills larynx.
Radiological exploration of the larynx
Modern imaging allows the exploration of the deep structures of the larynx.
The scanners provide excellent reconstructions in sagittal and frontal planes. The assessment of neoplastic diseases, certain rare conditions (laryngeal tuberculosis, laryngocele …) and the trauma of the larynx and laryngeal stenosis were the main indications.
But the main interest in imaging of the larynx on the evaluation of cancer (TNM staging, treatment choice).
The AP and lateral radiographs keep interest in the search for foreign bodies.
d.Diagnostic etiological
d.1-laryngitis
 Laryngitis red (cordite)
Laryngitis red (cordite)
D.1.a-laryngitis in adults
Frequent and often trivial, they are happy secondary to irritation by environmental factors (dust, toxic fumes, infectious agents …).
There is a potential risk of cancer in chronic laryngitis.
Acute laryngitis
They are most often viral. Dysphonia or aphonia installs quickly in an infectious context more or less marked with a dry cough. The vocal cords are hyperaemic with small vessels on their upper surface (catarrhal laryngitis).
The evolution is rapid, with regression on treatment within 48 hours, and return to normal larynx in 8 days.
Chronic laryngitis
The epithelium of the vocal chords will change from hyperplasia, dyskeratosis, or squamous metaplasia. Changes can be made to the term carcinogenesis through all stages of dysplasia.
Clinically the voice is hoarse, with abnormal fatigue late in the day but has been evolving for several weeks or months without improvement.
It is recognized classic and schematically two types of chronic laryngitis:
Laryngitis red realize hypervascularization resume broadcasts, sometimes with a submucosal swelling strings giving a blow.
Laryngitis white can also make several presentations endoscopic (leukoplakia, laryngitis pachyderm, horny papillomavirus)
Sometimes white and red lesions can coexist simultaneously.
These can sometimes fit into laryngitis systemic diseases (amyloidosis, sarcoidosis) or meet in tuberculosis.
These lesions include chronic laryngitis white imperatively require control histological (biopsy under general anesthesia).
d.1.b- laryngitis-child
Dysphonia is of secondary importance compared to the difficulty breathing.
Although common and benign laryngitis child can take a turn sometimes disturbing with respiratory distress due mainly to the reduced diameter of the laryngeal channel.
We recognize two main types of laryngitis in children:
The most common and fortunately the month is a severe subglottic laryngitis.
Viral it is manifested typically by a barking cough at night (“dog’s cough”) with dyspnea of varying importance. Dysphonia is in order very discreet because the inflammation is mainly subglottic topography.
The outcome was favorable in most cases anti-inflammatory treatment. Intubation is exceptional.
The most severe form is actually a haemophilus influenzae septicemia with abscess epiglottis. This is the very serious epiglottitis who has one antibiotic and anti-inflammatory in large emergencies. The clinical picture is that of a sudden dyspnea with laryngeal hupersalivation. The voice is stifled.
The child sits with a hyperthermic draw supraclavicular and suprasternal.
In the absence of early treatment decompensation can occur at any time.
d.2-pure organic or functional pathology begining
There are usually a concept of vocal burnout
These alterations of the mucosa of the vocal cord produced or maintained by a faulty vocal behavior.
D.2.a. Road-acquired injuries
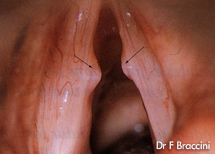 Nodules “kissing Nodules”
Nodules “kissing Nodules”
They are mainly in women and children (malmenage vocal). Localized in spaceREINKE, they respond to swelling and come in the form of small pearly white swellings, sometimes slightly pinkish, projecting from the free edge of the CV. They are usually bilateral, located at the junction of middle 1 / 3 and 1 / 3 anterior of the vocal cord, one in front of the other (“kissing nodules”).
Polyps

Polipi
They are mainly adult males, and are responsible for dysphonia more or less marked but permanent.
On the etiology often found the concept of malmenage vocal effort with closed glottis.
On the endoscopic, they translate as a pseudotumor rounded, happy angiomatosissometimes sessile with a broad base of implantation of the vocal cord or on the contrary pedunculated.
Unilateral their seats is much more variable than that of nodules, they are often at the union third-earlier third way, they can sit perfectly at the anterior commissure, in the middle of cv or even back in the arytenoid region.
Reinke edema
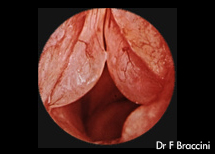
Si tratta di una malattia cronica della lamina propria gonfiore edematoso del CV, con una conseguente deformazione della superficie superiore ed il bordo libero.
Condizione comune si osserva soprattutto nelle donne e quasi esclusivamente fumatrici.
In endoscopia, CV è la sede di un gonfiore bianco o traslucido, gelatinoso, sessili. Massima è raggiunta l’aspetto classico della “vescica natatoria”.
In caso di grande gonfiore a vedere il classico Husky possibile combinare gravi episodi di dispnea inspiratoria fortunatamente sensibile agli anti-infiammatori.
La particolarità di questo (effetto è indotta dal fumo)’. Si dovrà quindi diffidare di cancro glottico associati.
Pathology of the Posterior Glottis
The most common injury is represented by the posterior granuloma of the glottis, usually secondary to prolonged intubation responsible for mucosal tear.
These granulomas usually do, despite their size, a very moderate dysphonia, or when a very large gene with breathing or swallowing.
Gastroesophageal reflux disease (GERD) should also be mentioned whenever there is inflammation of the posterior glottis (diffuse redness of the arytenoids).
The arytenoid ulcer (or ulcer Chevalier Jackson) sits mostly in the inner part of the arytenoid. It should also be mentioned first of GERD, but will have to find a zinc deficiency.
Juvenile laryngeal papillomatosis
This is a disease caused by a virus (papilloma virus), which affects children or young adults and is characterized by localized proliferation of the epithelium of the vocal cords to be true “clusters” .
In case of significant development of these clusters, they may be responsible for difficulty breathing (dyspnea), which makes the severity of the condition.
Malignant degeneration, although classical, is exceptional.
d.2.b-The congenital lesions of the vocal cords (cysts, sulcus glottidis, stretch marks)
Endoscopic diagnosis is often difficult without the use of the stroboscope or examination under a microscope, these lesions may be unilateral or bilateral, with no major signs of inflammation.
There is often an associated injury dysfunctional because of voice-induced forcing.
There is a special fatigability of the voice, resulting in a decline in the quality of vocal timbre at every opportunity.
There are still a decrease in vocal intensity, and brief moments of désonorisation corresponding to the so called most often holes in his voice.
d.3-recurrent paralysis (RP)
Common condition of the vocal cord paralysis is manifested by dysphonia (bitonal characteristic way) and swallowing disorders whose importance depends on the location of the asset.
If the rope is stuck open, the air leakage is a major loss of voice and aspiration of food (cough liquid) that make any immediate gravity.
However, if the vocal cord is blocked during closing (the midline), the symptoms are rough, dominated by dysphonia. The roads are false because there are so absent an effective glottic occlusion.
The causes are many and varied.
The most common surgical procedures are represented by the thyroid surgery, the left lung, the carotid arteries, but other causes can be found as a tumor (thyroid, mediastinum, esophagus, trachea), as traumatic, viral or idiopathic.
Apart from the etiological problem severity of PR is related to the risk of aspiration pneumonia.
d.4-organ damage Maligne
Cancer unilateral vocal cord
Especially in men, smoking, (ethyl), the etiology is suspected he joins in dyspnea, dysphagia, or otalgia reflex. The glottic laryngeal cancer can be pure or pharyngolaryngeal. Macroscopically, it can take a look budding or ulcers, with or without a mobility impairment, but sometimes it is the deceptive nature of laryngitis, suspicious, especially if the vocal cords have a whitish irregular, making the laryngitis elephantine white. This requires an endoscopy under general anesthesia with direct laryngoscopy in suspension and biopsies. I It is, in most cases of squamous cell carcinoma. The prognosis is good if the diagnosis is early. Any delay diagnosis may deprive the patient of conservative surgery and will fall life-threatening.
d.5-Aside
Other conditions which the list is not exhaustive may also cause dysphonia during their evolution:
-Injuries of the larynx (external trauma, surgery pharyngolaryngeal)
-The neurological diseases (Parkinson’s disease, amyotrophic lateral sclerosis, dystonia, laryngeal ….)
-Psychiatric illness [schizophrenia, depression (monotone), hysteria (aphonia), manic excitement (forcing voice)]
– The system diseases (rheumatoid arthritis, granulomatous …) or infectious (syphilis, tuberculosis …)
IV-Treatment of dysphonia
a.La speech therapy
Essential pillar of the treatment of voice disorders, speech therapy most often surrounds every move of phono-functional surgery.
His approach is also very different in case of malignancy (trouble swallowing, esophageal speech).
We will consider here that the rehabilitation of benign pathologies of the voice.
Sessions (minimum of 20) exceptions occur therapist’s office with a daily training that the subject continues at home. The duration of sessions should not be less than 30 minutes. It provides advance information on the anatomy and the mechanisms that govern the voice. It is also important to highlight the factors that lead to malmenage and forcing voice. The therapist must continually adapt to the personality of the patient while monitoring the technical aspects of rehabilitation.
The treatment of functional disorders caused by laryngeal paralysis is
be as early as possible, and always conducted in parallel with the etiological research.
Rehabilitation (2 to 3 sessions per week) aims to fight against muscle atrophy and prevent ankylosis of cricoarytenoid joint.
It “forces” the vocal cord valid beyond the midline to achieve a satisfactory glottal closure and avoid food aspiration. To achieve rehabilitation focuses mainly on sound systems accompanied by laryngeal manipulation.
This work is rewarding because it gives good results but in the absence of recovery after 8 months of medialization surgery may be considered.
In case of benign disease dysfunctional (nodule, polyp …), it works more gradually (1 to 2 sessions per week). Rehabilitation takes place in two parts.
A general part-oriented relaxation (master level of inner tension), the static (posture correction) and breath (costo-diaphragmatic breathing, work of the expiration).
A second part more specifically, with massages voice, voice placement and projection.
If it fails again we may have surgery.
b. The Medical Treatments
It is essential for the prescription of antibiotics and / or anti-inflammatory systemically and / or local. Anti-reflux treatment can be very useful in case of irritation of the glottis later.
c.La Surgery
In case of benign dysfunctional
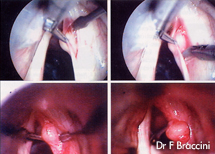
Phono
Excision of epidermal cyst under endoscopic control
The phono-surgery based on endoscopic instrumentation with conventional or laser.
Surrounded by a vocal rehabilitation effective functional surgery of the larynx that produces good results after excision of polyps, nodules or granulomas.
By contrast, the phono-surgery of Reinke edema and congenital lesions gives poorer results.
If a vocal cord paralysis in abduction
The techniques used aim to bring the midline vocal cord opening blocked. This medialization can be done endoscopically or cervicotomy side.
In case of malignancy
Surgery can be done endoscopically (cordectomie) for small lesions.
In case of larger lesions surgery will be more aggressive than the lesions are extensive.
Partial surgery of the larynx that allows for removal of the cancer while preserving a crossroads aero-digestive tract can not be seen until the disease has not stopped the vocal cord. And if made available in the neoplastic areas para-voice, responsible for a blockage of the vocal cord only a total laryngectomy may be considered.
This intervention is mutilating after tumor removal to sacrifice the larynx. Reconstruction establishes two distinct pathways for feeding and breathing (tracheostomy final).Learning a new voice is done by eructation (esophageal speech) or by the use of voice prostheses.
d. The other treatments
-Radiation therapy and chemotherapy respond to oncological indications of organ preservation or in addition to surgery.
L-interferon is sometimes used to treat laryngeal papillomatosis.
-The etiological treatment of a causal condition is also essential.
V-Conclusion
Dysphonia is a very common symptom for consultation both in the GP than in ENT.
Most often related to a dysfunctional home, it should nevertheless in case of persistent beyond one month still to eliminate an underlying neoplastic disease with functional and vital prognosis depends on rapid diagnosis.
 Article published in the medical assistance
Article published in the medical assistance
F Braccini, R Braccini, Saban Y.
What to do before a dysphonia.
Concours Médical 2001; 34, 2288-93.
* Frédéric Braccini, Rosine Braccini **, Yves SABAN *.
* ENT – Neck Surgery
4 avenue Georges Clemenceau – 06000 NICE
**